- Quick Answer
- What a Herniated Disc Actually Is
- Symptoms and How It Shows Up Day to Day
- What Contributes to a Herniated Disc
- Red Flags: When to Skip the Chiropractor and Seek Urgent Care
- How We Assess Your Case
- Your Personalized Treatment Plan
- What the Research Says
- Case Study: A Real Recovery Path
- Ready to Get Evaluated? Here Is What Happens Next
- Meet Your Doctor
- What Our Tucson Patients Say
- Watch: What Is a Herniated Disc? Causes, Exam, and Non-Surgical Relief
- Free Printable Recovery Guide
- Find Out If Your Symptoms Point to a Herniated Disc
- References and Medical Review
- Frequently Asked Questions

Herniated Disc Treatment in Tucson — Non-Surgical Relief That Works
Table Of Contents
-
-
- Quick Answer
- What a Herniated Disc Actually Is
- Symptoms and How It Shows Up Day to Day
- What Contributes to a Herniated Disc
- Red Flags: When to Skip the Chiropractor and Seek Urgent Care
- How We Assess Your Case
- Your Personalized Treatment Plan
- What the Research Says
- Case Study: A Real Recovery Path
- Ready to Get Evaluated? Here Is What Happens Next
- Meet Your Doctor
- What Our Tucson Patients Say
- Watch: What Is a Herniated Disc? Causes, Exam, and Non-Surgical Relief
- Free Printable Recovery Guide
- Find Out If Your Symptoms Point to a Herniated Disc
- References and Medical Review
- Frequently Asked Questions
-
Last Reviewed By: Dr. Christopher Cox, D.C., May 12, 2026
Quick Answer
A herniated disc happens when the soft inner material of a spinal disc pushes through a tear in its outer wall, often pressing on nearby nerves. Most cases are triggered by a mix of repetitive strain, lifting, poor mechanics, and the normal wear that comes with age. The good news: research consistently shows that the majority of people improve with conservative care in the first six to twelve weeks, without surgery. First-line options include activity modification, targeted chiropractic care, spinal decompression, specific exercise, and in some cases adjunct therapies like shockwave. Seek urgent medical care right away if you experience loss of bowel or bladder control, saddle numbness, progressive leg weakness, or severe pain after a significant trauma.

What a Herniated Disc Actually Is
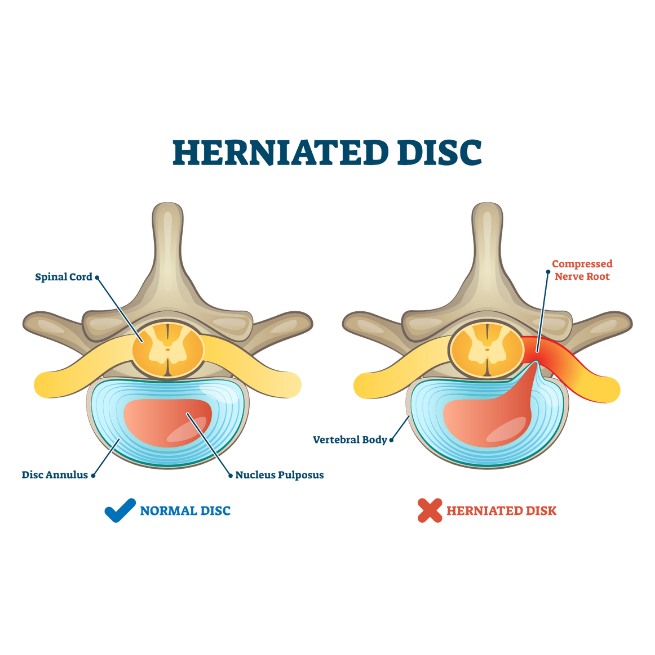
Your spine is built from 24 movable bones stacked on top of each other, separated by cushiony discs that act as shock absorbers. Each disc has a tough outer ring called the annulus fibrosus and a gel-like center called the nucleus pulposus. When that outer ring develops a weak spot or a tear, some of the inner gel can push outward. That is a herniated disc. You might also hear it called a bulging disc, slipped disc, ruptured disc, or disc protrusion. They all describe different stages of the same basic problem.
Most herniations happen in the lower back (lumbar spine), especially at the L4 to L5 and L5 to S1 levels, because that region carries the most load. The neck (cervical spine) is the second most common location. When the herniated material pushes against a nearby nerve root, it can cause pain, numbness, tingling, or weakness that radiates into the arm or leg. This is what most people mean when they say sciatica or a pinched nerve.
Herniated discs can be acute, triggered by a single event like a lifting injury or a car accident, or they can develop gradually over months and years as the disc slowly degenerates. Both respond well to conservative care in most cases, but the treatment plan looks different depending on how long you have been dealing with it.
Two Myths Worth Clearing Up
Myth one: a herniated disc means you need surgery. In most cases, you do not. Landmark research on lumbar disc herniation has shown that patients treated non-surgically often reach similar long-term outcomes to those who have surgery, and a large portion of herniations actually shrink or reabsorb on their own over time.
Myth two: if your MRI shows a herniation, that is definitely the cause of your pain. Not always. Studies have found that a meaningful percentage of pain-free adults have disc bulges, protrusions, and degeneration visible on imaging. That is why a good clinical exam matters so much. The MRI is one piece of the puzzle, not the whole answer.
Aggravating and Easing Patterns
Lumbar herniations typically feel worse with sitting, forward bending, lifting, and long drives. Standing and walking often feel better, at least in short bursts. Cervical herniations often flare with looking up, carrying bags on one shoulder, or long stretches at a computer. Lying down tends to ease pressure on the disc, which is why many people feel their best in the morning and worse as the day wears on.
How It Affects Real Life
Patients tell us herniated disc pain rarely stays neatly in the background. It interrupts sleep, shortens workouts, and turns simple things like putting on socks, grocery shopping, or sitting through a meeting into a mental calculation. Many people start avoiding activity altogether, which unfortunately makes the problem worse over time. Your body needs movement to heal. The goal of care is to get you moving safely again, not wrap you in bubble wrap.
Symptoms and How It Shows Up Day to Day
Herniated disc symptoms depend heavily on where the herniation is and whether a nerve is involved. Some people feel mostly local back or neck pain. Others feel very little back pain but intense symptoms radiating into an arm or leg.
Common Symptoms
- Sharp, burning, or shooting pain down one leg (sciatica) or one arm
- Numbness or tingling in the foot, toes, hand, or fingers
- Muscle weakness, such as difficulty lifting the foot or gripping objects
- Deep aching in the lower back or between the shoulder blades
- Pain that worsens with coughing, sneezing, or bearing down
- Stiffness first thing in the morning or after sitting for long periods
What Contributes to a Herniated Disc
There is rarely one single cause. In most patients, a herniated disc is the result of several contributors stacking up over time until the disc can no longer handle the load.
Mechanical and Load Factors
- Repetitive lifting, bending, and twisting (especially in construction, nursing, warehouse, and delivery work)
- A single heavy lift with poor technique
- Falls, sports injuries, or motor vehicle accidents
- Prolonged sitting with rounded posture, which increases pressure on lumbar discs
- Previous spinal injuries that changed how you move
Lifestyle Contributors
- Deconditioning and weak core or hip musculature
- Smoking, which reduces blood flow to the disc and slows healing
- Carrying excess body weight, which increases daily spinal load
- Chronic dehydration, since discs rely on hydration to stay resilient
- Poor sleep and high stress, both of which lower pain tolerance and slow tissue recovery
Capacity Versus Demand
A useful way to think about it: your spine has a certain capacity for load at any given moment, and your life places certain demands on it. When demand outpaces capacity, tissues fail. Sometimes the fix is to lower the demand for a short window. Often the better long term fix is to build more capacity through targeted strengthening, mobility work, and smarter movement patterns. Most of our care plans work on both sides of that equation at once.

Red Flags: When to Skip the Chiropractor and Seek Urgent Care
Most herniated discs are not medical emergencies. A small number are. If you notice any of the following, go to an emergency department or call 911 right away. Do not wait for a chiropractic appointment.
- New loss of bowel or bladder control, or difficulty urinating
- Numbness in the saddle area (inner thighs, groin, buttocks)
- Progressive weakness in one or both legs, or foot drop
- Severe pain following a significant trauma such as a fall from height or a serious car crash
- Unexplained fever, chills, or night sweats along with back pain
- Unexplained weight loss, a history of cancer, or suspected infection
- Severe pain that is not relieved at all by lying down
These signs can point to cauda equina syndrome, fracture, infection, or other conditions that need immediate imaging and, in some cases, emergency surgery. Conservative care is not appropriate until those are ruled out. As Dr. Cox often says, if we are not the right fit for your case, we will tell you who is.
How We Assess Your Case
A good treatment plan starts with a good assessment. Before any adjustments, any decompression sessions, or any exercise prescription, we need to understand what is actually driving your pain. Our evaluation is built to answer three questions: what is the likely source, is it safe for conservative care, and what is the best starting point for you specifically.
Detailed History
We talk through when the pain started, what you were doing when it began, how it has changed, what makes it better and worse, what you have already tried, your work and sleep habits, your previous injuries, and your overall health. This conversation alone tells us a great deal.
Physical and Neurological Exam
We check spinal range of motion, posture, and movement quality. We palpate the spine and surrounding muscles. Most importantly for suspected disc cases, we perform neurological testing: reflex testing, muscle strength testing across key nerve roots, sensory testing for numbness or tingling, and orthopedic tests like the straight leg raise, slump test, and Spurling test that help localize nerve root involvement.
Functional Movement Screening
How you sit, stand, bend, squat, and load your spine under real tasks often reveals more than an isolated range of motion measurements. We look for the patterns that are feeding your pain so we can change them.
Differential Diagnosis
Not every radiating leg pain is a disc. It could be piriformis syndrome, SI joint referral, facet joint pain, spinal stenosis, hip pathology, or peripheral nerve entrapment. Part of a thorough assessment is ruling those in or out so the plan actually targets the right problem.

Imaging: When It Is Needed, and When It Is Not
Current clinical guidelines recommend against rushing to MRI in the first four to six weeks of low back pain unless red flags are present or there is significant, progressive neurological involvement. Imaging too early can lead to unnecessary treatments, more worry, and sometimes more aggressive interventions that were not needed in the first place. If your case warrants imaging, we will tell you clearly and coordinate with your medical doctor or a specialist in our referral network.
Your Personalized Treatment Plan
We use a phased care ladder that meets you where you are and progresses only when your body is ready. No two plans look exactly alike, but the overall structure gives patients a clear sense of where they are in the recovery process and what comes next.
Phase 1: Calm the Irritation
The first goal is to quiet the pain and calm the inflamed nerve. Depending on your case, this may include gentle, precisely targeted chiropractic adjustments (we do not crank or aggressively twist acute disc patients), positional relief strategies, icing guidance, activity modification, and non-surgical spinal decompression when indicated. Many patients feel noticeable relief within the first two to three weeks, though the underlying disc still needs time to heal.

Phase 2: Restore Normal Motion
Once irritation is settling down, we shift focus to restoring normal movement through the involved segment and the regions above and below it. The spine works as a chain. If the hips are stiff or the mid back is locked up, the lumbar spine ends up taking the hit. This phase blends manual therapy, mobility work, soft tissue techniques, and early corrective exercise.
Phase 3: Rebuild Capacity
This is where most patients start to feel like themselves again, and it is the phase people most often skip if they are not in a structured plan. The goal here is to strengthen the deep core, hips, glutes, and spinal stabilizers so the disc is no longer carrying loads it was not designed to handle. Without this step, a lot of people get better and then reinjure themselves a few months later.

Phase 4: Return to the Life You Actually Want
Pain-free sitting at a desk is one thing. Lifting your grandkids, hiking Sabino Canyon, or getting back on the pickleball court is another. Phase 4 is about translating strength and mobility into real-world tasks so the progress sticks. We also lay out a simple maintenance plan so small flare ups do not turn into full relapses.
Adjunct Technologies We May Use
Not every tool is right for every case. We select adjuncts based on your specific presentation, tissue tolerance, and goals. Options we have in-house include:
- Non-surgical spinal decompression, which gently stretches the spine to reduce pressure on discs and nerves
- Shockwave therapy for chronic soft tissue involvement and stubborn surrounding muscle dysfunction
- Custom orthotics when foot mechanics are contributing to lumbar load
- Targeted rehab exercise tailored to your phase of recovery
Clinical note: Not every modality is right for every patient, and we will never stack therapies just to fill a visit. If a treatment is not indicated for your specific case, we will tell you and leave it out. If another provider, specialist, or surgeon is the better fit for where you are at, we will tell you that too.

What the Research Says
Herniated disc care is one of the most heavily researched areas in musculoskeletal medicine. Here is a plain-language summary of what the most relevant, high-quality evidence actually suggests. Full references are listed at the bottom of this page.
ACP Clinical Practice Guideline (2017) on Low Back Pain
What it suggests: Recommends non-drug, non-surgical treatments as first-line care for most acute, subacute, and chronic low back pain, including spinal manipulation, exercise, and other conservative options. Who it applies to: Adults with non-specific low back pain, including many cases involving disc involvement. Limitation: Guideline does not cover every subtype of radiculopathy and does not replace individual clinical judgment.
SPORT Trial (Weinstein et al., JAMA 2006)
What it suggests: Compared surgery to non-operative care for lumbar disc herniation. Both groups improved significantly, and long-term outcomes were similar, though surgery offered faster initial relief in some patients. Who it applies to: Adults with confirmed lumbar disc herniation and radiculopathy who were surgical candidates. Limitation: Patients were not strictly randomized throughout, and results do not apply to every disc scenario.
JAMA Systematic Review on Spinal Manipulation (Paige et al., 2017)
What it suggests: Found that spinal manipulative therapy is associated with modest improvements in pain and function for acute low back pain, with a low rate of serious adverse events when delivered by trained providers. Who it applies to: Adults with acute low back pain, including some presentations with radiating symptoms. Limitation: Effect sizes are modest, and the review emphasized combining manipulation with other active care.
Imaging Findings in Asymptomatic People (Brinjikji et al., AJNR 2015)
What it suggests: Found that disc bulges, protrusions, and degeneration are common on MRI in people without any back pain, and the prevalence increases with age. Who it applies to: General adult population across a wide age range. Limitation: Does not mean imaging findings are irrelevant, only that they must be interpreted alongside a clinical exam.
NICE Guideline (NG59) on Low Back Pain and Sciatica
What it suggests: Recommends self-management, exercise, manual therapy as part of a treatment package, and psychological support, while discouraging routine imaging and early opioid use. Who it applies to: Adults in the UK healthcare system with low back pain and sciatica, though principles are widely applied internationally. Limitation: Developed in a different healthcare system, so some recommendations around access and referral pathways may not map exactly to US care.
Taken together, the evidence points in a consistent direction: for most people with a herniated disc, a well-structured, active, conservative care plan should come before injections or surgery. Surgery is absolutely the right answer for some cases. It just is not the right first step for most.
Case Study: A Real Recovery Path
The following case is a de-identified composite based on typical patients we see at our Tucson clinic. Details are adjusted to protect privacy.
Patient Profile
A 47-year-old warehouse team lead from east Tucson who had been dealing with worsening low back and right leg pain for about three months after a lifting incident at work. He had tried over-the-counter anti-inflammatories, a heating pad, and rest. Pain was starting to wake him up at night and was limiting his ability to drive to job sites.
Baseline Limitations
- Pain rated 7 out of 10 at its worst, typically 4 to 5 out of 10 during the day
- Unable to sit longer than 15 minutes without shifting or standing
- Tingling into the right calf and outer foot
- Could no longer play pickup basketball, and had cut back on time with his kids
- Sleep interrupted 2 to 3 times per night
Assessment Findings
History and exam were consistent with a right-sided L5 to S1 disc involvement with early nerve root irritation. No red flags were present. Reflexes and strength were intact, though sensation was mildly reduced over the outer right foot. Orthopedic testing reproduced his familiar leg pain.
Plan and Duration
Eight weeks of structured care, starting with three visits per week and tapering as he improved.
Interventions Used
- Gentle, low-force chiropractic adjustments targeted to the lumbar and pelvic regions
- Non-surgical spinal decompression sessions two to three times per week early on
- Soft tissue work to the glutes, hip rotators, and lumbar paraspinals
- Progressive rehab exercise starting with nerve glides and core stabilization, building into hip hinge and loaded carry work
- Ergonomic coaching for truck driving and warehouse lifting
- Simple home routine of 10 to 15 minutes, most days
Milestones
Week 2: Leg pain intensity cut roughly in half. Sleep interruptions down to once per night. Week 4: Tingling in the foot largely resolved. Sitting tolerance up to 45 minutes. Back to light basketball shooting, no pivoting yet. Week 8 and beyond: Pain reported at 0 to 1 out of 10 most days. Full return to work duties. Returned to pickup basketball with confidence in his body.
Outcome Metrics
- Pain score improvement from 7 out of 10 to 0 to 1 out of 10
- Oswestry-style functional scores moved from moderate disability to minimal
- Returned to all desired work, family, and recreational activities
- Reported high confidence in managing future flare ups
Maintenance Plan
Monthly check-ins for the first three months post-recovery, then as-needed care. A short daily mobility routine, twice-weekly strength work, and a simple flare-up protocol he could run himself if a rough day showed up.

Ready to Get Evaluated? Here Is What Happens Next
If you have been dealing with back pain, leg pain, or a diagnosis of a herniated disc and you are not sure what to do next, we would be glad to take a careful look at your case. Our approach is built around complex and chronic problems, which is exactly what many disc cases turn into when they do not get the right plan early.
What Your First Visit Looks Like
- A one-on-one consultation with Dr. Cox or a member of our clinical team
- A thorough history and physical exam, including neurological testing
- A clear explanation of what we think is going on, in plain language
- An honest recommendation, whether that is care with us, a referral to a specialist, or simply some reassurance and a few things to try at home
- A transparent conversation about what care would involve, including cost and financing
If we are the right fit, we will build you a plan. If we are not, we will tell you exactly who is. That has been our commitment to the Tucson community for more than two decades.
Serving patients across Tucson, Vail, Oro Valley, Marana, Sahuarita, and surrounding Southern Arizona communities.
Book Your Consultation
Meet The Team





What Our Patients Are Saying
What Is a Herniated Disc? Causes, Exam, and Non-Surgical Relief
Download our Free Printable Recovery Guide
Want something you can print, stick on the fridge, and actually use? Our free Herniated Disc Recovery Guide walks you through what to do in the first two weeks, which positions to avoid, simple movements that are usually safe, and a checklist of red flags to watch for.
What Is Inside
- A clear, one-page overview of what a herniated disc is and is not
- Safe positions and postures for sleeping, sitting, and working
- A short list of movements to try, and a list of things to avoid in the early phase
- Red flag checklist so you know when to escalate to urgent care
- A simple tracker so you can see your progress week by week

Find Out If Your Symptoms Point to a Herniated Disc
References and Medical Review
References
- Qaseem A, Wilt TJ, McLean RM, Forciea MA, for the Clinical Guidelines Committee of the American College of Physicians. Noninvasive Treatments for Acute, Subacute, and Chronic Low Back Pain: A Clinical Practice Guideline From the American College of Physicians. Ann Intern Med. 2017;166(7):514 to 530.
- Weinstein JN, Tosteson TD, Lurie JD, et al. Surgical vs Nonoperative Treatment for Lumbar Disk Herniation: The Spine Patient Outcomes Research Trial (SPORT): A Randomized Trial. JAMA. 2006;296(20):2441 to 2450.
- Paige NM, Miake-Lye IM, Booth MS, et al. Association of Spinal Manipulative Therapy With Clinical Benefit and Harm for Acute Low Back Pain: Systematic Review and Meta-analysis. JAMA. 2017;317(14):1451 to 1460.
- Brinjikji W, Luetmer PH, Comstock B, et al. Systematic Literature Review of Imaging Features of Spinal Degeneration in Asymptomatic Populations. AJNR Am J Neuroradiol. 2015;36(4):811 to 816.
- National Institute for Health and Care Excellence (NICE). Low back pain and sciatica in over 16s: assessment and management. NICE Guideline NG59. Published 2016, updated thereafter.
- Bronfort G, Haas M, Evans R, Leininger B, Triano J. Effectiveness of manual therapies: the UK evidence report. Chiropr Osteopat. 2010;18:3.